Healthy Youth = Healthy families = healthy Community
Training young people to build skills to maintain a healthy self, healthy relationships, and healthy future has a huge impact on building healthy families and healthy communities.
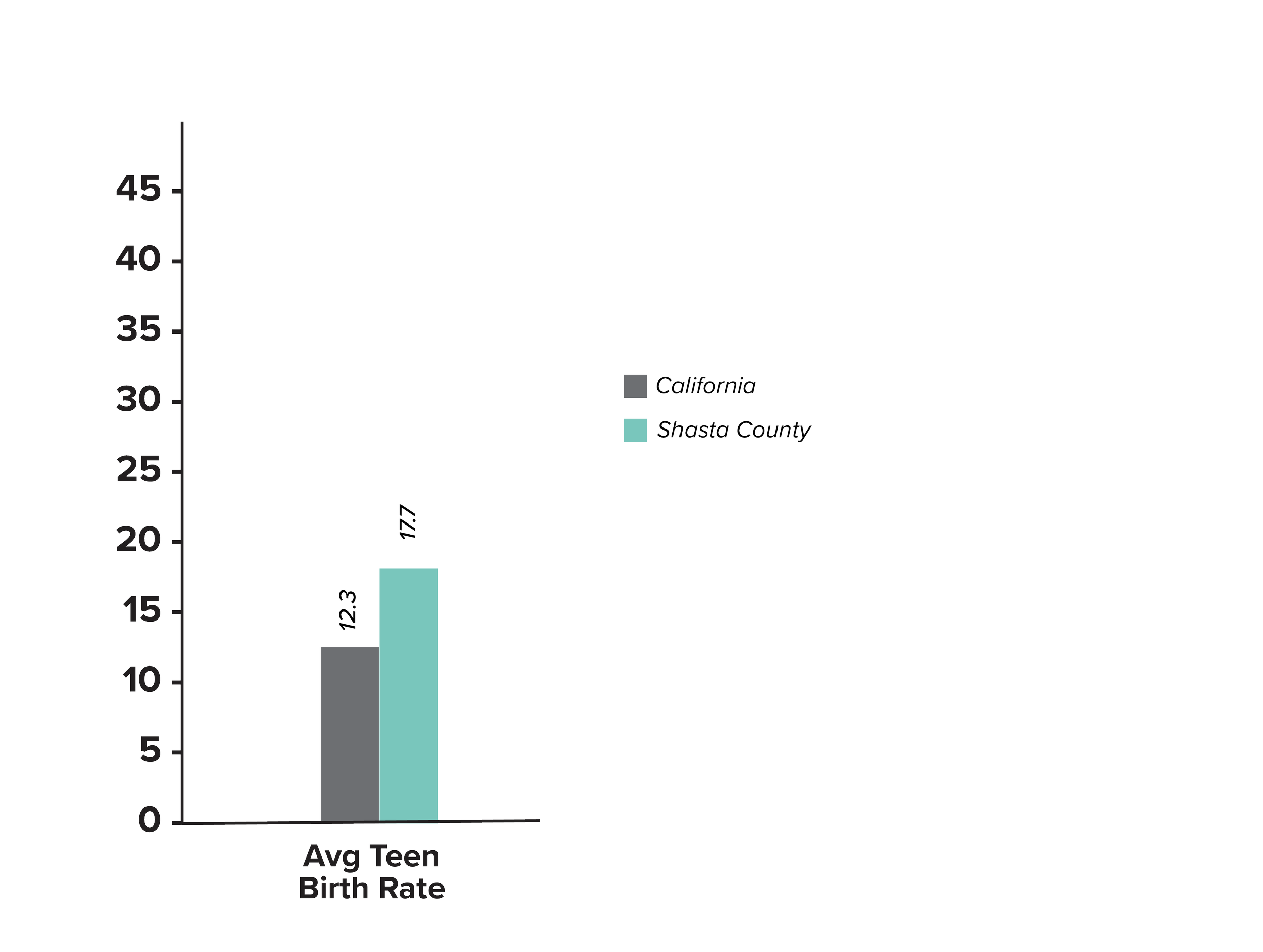
Shasta County Health and Human Services, in collaboration with other agencies, have been working to reduce risks and to expand efforts for prevention education in Shasta County. CYP wants to strengthen these efforts by making primary prevention education more accessible and readily available.